Appendix A: Supportive care
Appendix A: Supportive care
Supportive care in cancer refers to the following five domains:
- physical domain, which includes a wide range of physical symptoms that may be acute, relatively short-lived or ongoing, requiring continuing interventions or rehabilitation (NBCC & NCCI 2003)
- psychological domain, which includes a range of issues related to the person’s mental health and personal relationships (NBCC & NCCI 2003)
- social domain, which includes a range of social and practical issues that will affect the individual and their family such as the need for emotional support, maintaining social networks and financial concerns (NICE 2004)
- information domain, which includes access to information about cancer and its treatment, support services and the health system overall (NBCC & NCCI 2003)
- spiritual domain, which focuses on the person’s changing sense of self and challenges to their underlying beliefs and existential concerns (NICE 2004).
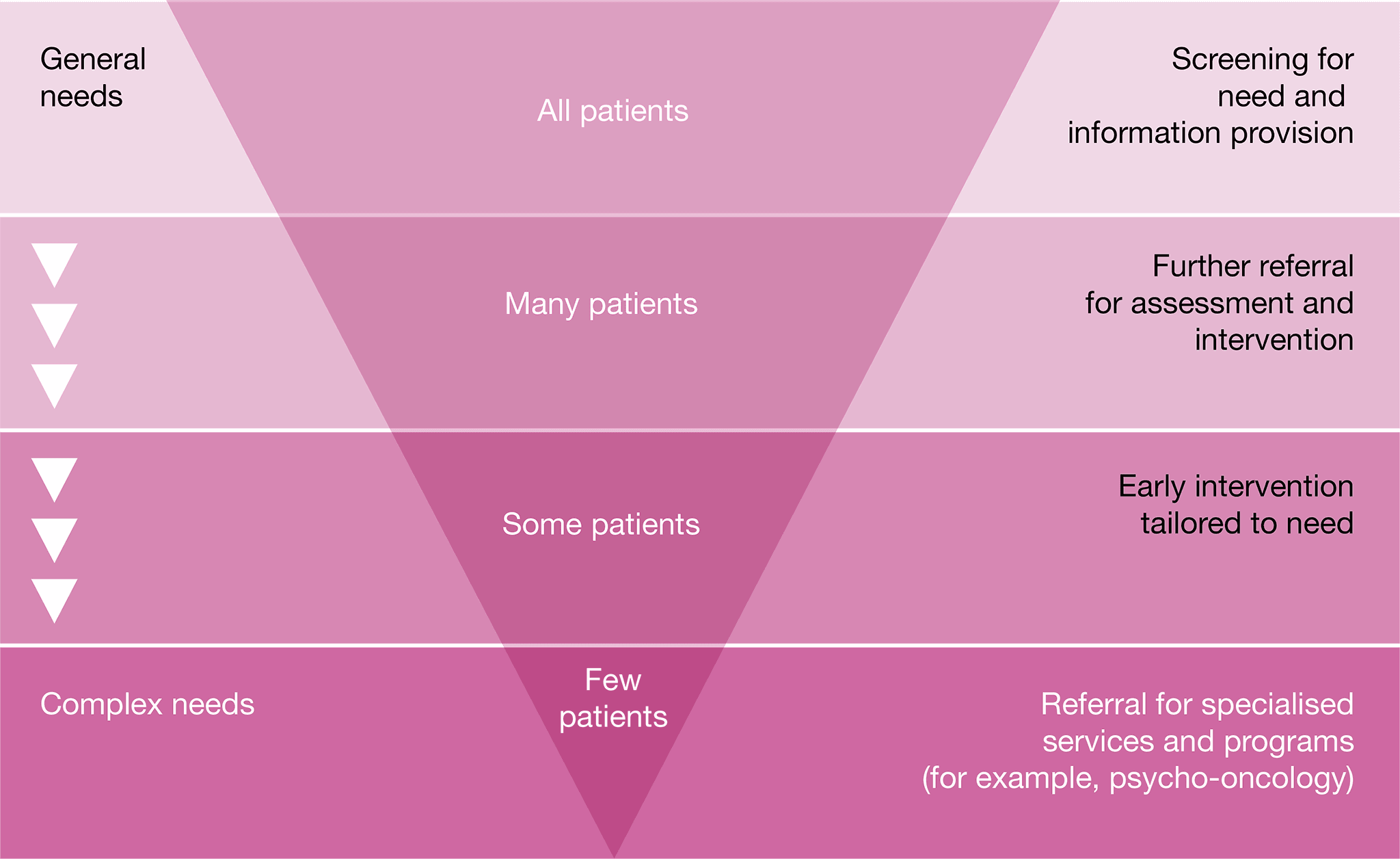
Fitch’s (2000) model of supportive care recognises the variety and level of intervention required at each critical point as well as the need to be specific to the individual. The model targets the type and level of intervention required to meet patients’ supportive care needs.
The tiered approach
Common indicators in patients with sarcoma who may require referral to appropriate health professionals and/or organisations include the following.
Physical needs
- Decline in functional status (particularly as a result of limb reconstruction or amputation) may affect the patient’s mobility and ability to take part in everyday activities. Referral to an occupational therapist, orthotist/prosthetist and a physiotherapist or exercise physiologist for assessment, education, intervention and compensatory strategies may assist with maintaining mobility. These may require prolonged periods of rehabilitation.
- Patients require ongoing nutritional screening, assessment and management. Consideration should be given to minimising the risk of late effects.
- Patients who have had an amputation require rapid and easy access to prosthetic services.
- Lymphoedema may require referral to a trained lymphoedema practitioner.
- Pain control should be proactively managed by referral to a pain management specialist.
- Symptoms of fatigue (physical and emotional) should be assessed and referred as necessary.
- Patients require ongoing nutritional screening, assessment and management. Reduced oral intake and/or swallowing difficulties and weight loss require referral to a dietitian and speech pathologist (for swallowing difficulties).
- Assistance from a pharmacist with managing complex medication regimens, multiple medications, assessing side effects and assistance with difficulties swallowing medications may be required.
Psychological needs
- Patients with sarcoma should be regularly screened for psychosocial needs including body image concerns, fear of the diagnosis and fear of recurrence, fertility, fatigue, existential anxiety, treatment phobias, anxiety/depression, interpersonal problems and sexuality concerns.
- Health professionals should be aware that stress and depression can be common in carers including family members. Advice and referral options should be discussed.
- If loss of independence is a factor contributing to depression, then referral to physiotherapy and occupational therapy may restore some independence and assist some people. Referral to a psychologist or psychiatrist may also be helpful in managing the depression.
- Disfigurement and scarring from appearance-altering treatment and the need for a prosthesis may require referral to a specialist psychologist, psychiatrist, orthotist/prosthetist or social worker.
- For people from culturally and linguistically diverse backgrounds, Aboriginal and Torres Strait Islanders, and lesbian, gay, bisexual, transgender and intersex (LGBTI) communities, a cancer diagnosis can come with additional psycho-social complexities. Access to expert health professionals may be required.
- Alteration in cognitive functioning can affect the patient’s ability to remember and maintain concentration. Strategies to help manage cognitive impairment, such as maintaining written notes or a diary, may be helpful.
- Fear of cancer recurrence is common in the post-treatment phase. Some people may have disabling symptoms and may benefit from referral to a psychology service.
- Consider a referral to a psychologist, psychiatrist or social worker if the patient is:
- displaying emotional cues such as tearfulness, distress, avoidance and withdrawal
- preoccupied with or dwelling on thoughts about cancer and death
- displaying fears about the treatment process and/or the changed goals of their treatment
- worried about loss associated with their daily function, dependence on others and loss of dignity
- becoming isolated from family and friends and withdrawing from company and activities that they previously enjoyed
- feeling hopeless and helpless about the impact that cancer is having on their life and the disruption to their life plans
- struggling with communicating to family and loved ones about the implications of their cancer diagnosis and treatment
- experiencing changes in sexual intimacy, libido and function
- struggling with the diagnosis of metastatic or advanced disease
- having difficulties transitioning to palliative care.
Social/practical needs
- A diagnosis of sarcoma can have financial, social and practical impacts on patients, carers and families.
- Significant restrictions to social activities may require referral to a social worker, occupational therapist, psychologist or psychiatrist.
- Practitioners should be aware of the implications of the diagnosis on schooling, education and employment.
- Practitioners should be aware of the impact of the diagnosis on sexual health and family planning.
- Help with legal issues may be required including for advance care planning, appointing a power of attorney, completing a will and making an insurance, superannuation or social security claim on the basis of terminal illness or permanent disability.
Information needs
- Use simple language and avoid jargon when talking with patients and their families.
- Provide written information and links to reputable websites to support verbal information given to patients and their families.
- Consider the need for appropriate information for people from culturally and linguistically diverse backgrounds.
- Fertility options should be discussed with the patient and/or family, where appropriate, before beginning treatment.
Spiritual needs
- Patients with cancer and their families should have access to suitably qualified, authorised and appointed spiritual caregivers throughout the cancer journey.






